Why Your Doctor Might Want You to Take a “Little Yellow Pill”
If you’ve been told your pregnancy is “high-risk,” one of the first things your doctor likely recommended was a daily low-dose aspirin. But if you’ve been doing your own research, you might have noticed a confusing debate: Should you take one baby aspirin (81mg) or two?
As a specialist in high-risk pregnancy (Maternal-Fetal Medicine), I see this question every day. Let’s break down the “Aspirin Revolution” and what it means for you and your baby.
The Goal: A Happy Placenta
To understand why aspirin matters, we have to look at the placenta. Think of the placenta as a high-tech “docking station” that connects your blood supply to your baby’s.
In a healthy pregnancy, the blood vessels are wide and relaxed, allowing oxygen and nutrients to flow easily. In some pregnancies, these vessels stay narrow and “tight.” This can lead to preeclampsia—a condition involving high blood pressure that can be dangerous for both mom and baby.
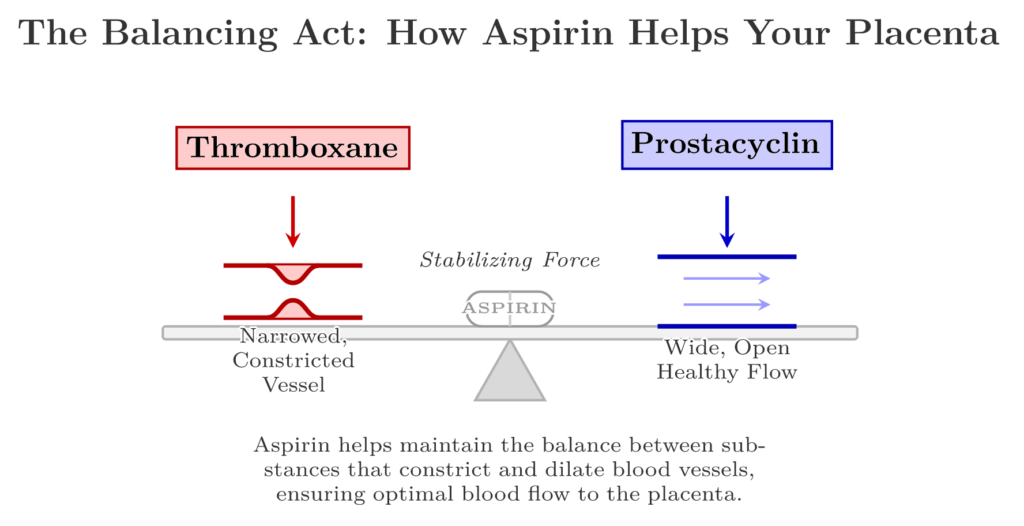
How Aspirin Helps: The “Teeter-Totter”
Inside your blood, there are two main “messenger” chemicals that play a game of tug-of-war:
- Thromboxane: The “Constrictor.” It makes blood vessels narrow and encourages clotting.
- Prostacyclin: The “Relaxer.” It keeps blood vessels open and blood flowing smoothly.
In preeclampsia, the “Constrictor” starts winning. Aspirin acts like a weight on the other side of the teeter-totter. It blocks the “Constrictor,” helping the “Relaxer” keep your blood vessels open and the placenta healthy.
The Big Debate: 81mg vs. 150mg
For decades, the standard advice in the U.S. has been one baby aspirin (81mg) a day. However, a major international study called the ASPRE Trial changed the conversation.
Researchers found that for women at high risk, a slightly higher dose—150mg (which is about two baby aspirins)—was significantly more effective at preventing early preeclampsia than a lower dose.
Why the higher dose?
- Body Size: We’ve learned that for some women, especially those with a higher BMI, one tiny pill might not be enough to get the job done.
- Better Protection: The higher dose seems to provide a “shield” that is more reliable at keeping those placental vessels open.
The “Bedtime” Secret
It’s not just how much you take, but when you take it. Research suggests that taking your aspirin at night works better. Your blood pressure naturally fluctuates on a 24-hour cycle, and taking aspirin before bed helps regulate your system while you sleep, providing better protection the next day.
Is it Safe?
This is the number one question I get. For the vast majority of patients, low-dose aspirin is incredibly safe. It does not cause the same issues as full-strength aspirin (like what you’d take for a severe headache), and it has been used in millions of pregnancies with a very strong safety record for both mom and baby.
What Should You Do?
Right now, U.S. guidelines still officially recommend 81mg. However, many specialists (including myself) are moving toward the higher dose for specific patients.
Questions to ask your MFM at your next visit:
- “Based on my history, am I a candidate for 150mg (two pills) instead of 81mg?”
- “Should I be taking my dose specifically at bedtime?”
- “When is the best time for me to start (usually between 12 and 16 weeks)?”
The Bottom Line
Aspirin is a small intervention that makes a massive difference. Whether it’s one pill or two, you’re taking a proactive step to support your placenta and give your baby the best environment to grow.